Clinical Hypnosis and Self-Regulation
I’m mostly taking notes on recreational applications of this text. I’m likely going to miss a lot of nuance in these articles, and then it’s going to be filtered through my writing. So uh - if you need this for something legit, go reference the actual journal articles.
Much like you wouldn’t consume Mind Play and take everything as fact, read this knowing this book’s subtitle is “Cognitive-Behavioral Perspectives,” accepting that as it’s lens and focus for understanding hypnosis.
Personally - while reading this book, I’ve felt my perspective slowly shift from “I wish they would stop attacking state theory so damn much” to “woah, look at these sick new tools.” Since it’s a cognitive-behavioral approach, they also took all the flavor and fun out of any of the suggestions. If you’re playing this game at home, it’ll be up to you to apply these ideas in a fun and approachable manner.
- Hypnosis: Cognitive-Behavioral Perspectives
- 1 - A Comprehensive Three-Dimensional Theory of Hypnosis
- 2 - Hypnotic Involuntariness and the Automaticity of Everyday Life
- 3 - Hypnotic Responding: A Cognitive-Behavioral Analysis of Self-Deception
- 4 - Whither Hypnosis? A Rhetorical Analysis
- 5 - Measures of Hypnotic Responding
- 6 - The Carleton Skill Training Program for Modifying Hypnotic Suggestibility: Original Version and Variations
- 7 - A Multimodal Framework For Clinical Hypnosis
- 8 - Clinical Hypnosis as a Nondeceptive Placebo
- 9 - Applying Hypnosis in Pain Management: Implications of Alternative Theoretical Perspectives
- 10 - Hypnosis and the Treatment of Smoking Cessation and Weight Loss
- 11 - Hypnosis and Forensic Psychology
- 12 - Self-Regulation Therapy - Suggestion Without Hypnosis
- 13 - Applications of Emotional Self-Regulation Therapy
Introduction
Section titled “Introduction”- Hypnotic psychodynamic treatments almost double their effectiveness compared to their non-hypnotic counterparts.
- Hypnotic treatments are extra effective for obesity.
- Fears and negative attitudes towards hypnosis can be a hinderance.
Clinical Hypnosis and Cognitive-Behavioral Psychotherapy
- Many behavioral therapies include relaxation, much like many hypnotic inductions. Given this, we can interchange relaxation with the induction, and start to introduce other cognitive behavioral strategies.
- ”… the rejection of the altered-state hypothesis is central to the cognitive-behavioral conception of hypnosis.”
- Given this, achieving trance is no longer an obstacle
- “hypnotic cognition can thus be seen as… explainable in terms of ordinary cognition”
The Altered-State Debate
- ”… most researchers now agree that hypnotic responses are not due to an altered state.”
- “The issue in the state debate was not what hypnosis does, but rather how it does it.” Sabrin’s Role Theory
- Sabrin suggested that hypnosis can be a role. “Role-taking is organismic,” it ‘embraces’ the entire organism, not just the voluntary systems.
- Sabrin also suggested that while some people understand and are motivated by the hypnotic role do not respond strongly, this is because of some lack of natural aptitude.
Barber’s Operational Paradigm
- TX Barber said there were eight components to hypnotic response… then later left out these eight components because they could replicate everything without an induction.
Later Cognitive-Behavioral Theory
- Spanos noted that the feeling of involuntariness in goal directed fantasies, leading towards self-deception.
- Kirsch argued that expectancy may be the most important component, as difficult phenomena (negative/positive hallucination) are not normally within someone’s cognitive abilities
The Collapse of State Theory
- Hilgard noted that the change in suggestibility after induction was minimal.
- Orne found that ‘simulators’ of hypnosis were prone to overplay their roles, in compared to individuals that went along with the hypnotic suggestions.
- Suggestible people continue to respond to hypnotic suggestions when alone (as shown by hidden cameras.)
- Hilgard proposed trance as a label for their subjective experiences, not a unique state.
- Woody and Bowers proposed a theory of dissociated control - where executive behavior was weakened, allowing suggestions to be more effective.
Neodissociation Theory: The Successor to Trance Theory
- Hilgard in later works hypothesized that part of the consciousness was unaware of what was going on.
- Hilgard also mentioned the hidden observer - which can also be used in a suggestion that part of them can be aware of something, and part of their awareness can be dissociated. People would report less of the suggested effect after mentioning the ‘hidden observer.’
- Spanos was able to modify the effects people were aware of by changing the suggestion of the hidden observer, later labeled the flexible observer. This found that hidden observer reports depended on the suggestion given (duh.)
- The book suggests that the correlation between dissociative tendencies of an individual and hypnotic response were found to be low.
The book…
- Part I - theoretical foundations.
- Part II - measurement and modification
- Part III - has an overview of multimodal psychotherapy
- Part IV - Devoted to self-regulation therapy, which works well for individuals with negative opinions towards hypnosis.
Hypnosis: Cognitive-Behavioral Perspectives
Section titled “Hypnosis: Cognitive-Behavioral Perspectives”1 - A Comprehensive Three-Dimensional Theory of Hypnosis
Section titled “1 - A Comprehensive Three-Dimensional Theory of Hypnosis”TX Barber
- There are three types of excellent hypnotic subjects. People absorbed to fantasy, the amnesia prone, and individuals with a positive view on hypnosis and it’s
Type 1: The Fantasy-Prone Person
Section titled “Type 1: The Fantasy-Prone Person”- Had paranormal or psychic experiences, including religious experiences
- Fantasy ability at an early age
- “Psychosomatic lability or plasticity” or “mind affecting body”
- “Vivid sexual fantasies… result in orgasms in 75% of these women.”
- Vivid personal memories prior to age 3
- From a young age, spent much of their time in fantasy.
Type 2: Amnesia-Prone
Section titled “Type 2: Amnesia-Prone”- Amnesia for hypnosis, as well as experiencing microamnesias during daily life.
- Sometimes called dissociaters, but this can be misleading, as the term is used differently between investigators.
- Most of these subjects (60%) experienced spontaneous amnesia for hypnosis. They were consistently able to experience post-hypnotic amnesia.
- Instead of remembering their suggested experiences as hallucinatory, they usually saw them as real.
- Poor memory of early life - as well as easily forget major events (like the contents of an engrossing book they just read.)
- Indications of childhood abuse.
- Interestingly, this category was not fantasy prone.
- Needed long inductions.
Type 3: The Positively-Set Person
Section titled “Type 3: The Positively-Set Person”- Positive attitudes, motivations, and experiences towards hypnosis.
- Were trusting and cooperative individuals, and were generally not negative, suspicious, or controlling.
- Expects and wants things to happen.
- Willing to let go and trust
- Able to infer ‘what the hypnotist requires.’
- Avoid irrelevant thoughts, trying to focus their attention on the suggestions.
- Feelings of enthusiasm, or feel something novel or unusual will happen.
Investigators Have Known One or Two of the Three Types
Section titled “Investigators Have Known One or Two of the Three Types”- Across cultures - there are two types of people that become shamans - the fantasy prone and the amnesia prone. Either one becoming lost in imagery, or the other becoming lost in an amnesiac experience (being possessed by a deity and forgetting the events.)
- Earlier in history - ‘hysterics’ tended to be amnesia and fantasy prone.
Reevaluation of Hypnotic Phenomena
Section titled “Reevaluation of Hypnotic Phenomena”Or - how these types of subjects will likely work with challenging suggestions.
Analgesia
Section titled “Analgesia”- Amnesia prone - Will block out the pain as they’ve blocked out traumatic events.
- Fantasy Prone - Will respond well to being guided into a fantasy where the pain is ignored.
- Positively Set - uses a wide variety of tools to reduce pain. (Attending to something else, reinterpretation, coping verbalizations, relaxation to reduce anxiety.)
Amnesia
Section titled “Amnesia”- Amnesia prone - “as real as real” amnesia with posthypnotic suggestion.
- Positively set - will self-distract, motivated unwillingness to recall, or other strategies.
- Fantasy prone - typically do not want to forget their experiences - unless they’re given suggestions that the amnesia is part of the fantasy. (Guided to fantasize ‘as real as real,’ awakening from anesthesia, or awakening from profound sleep.)
Age Regression
Section titled “Age Regression”- Fantasy Prone - naturals at this, can also imagine/experience past or future lives.
- Amnesia Prone - may be a poor subject for this. (This is a danger zone - if it works, it may be dramatic due to the aforementioned likely trauma.)
- Positively Set - middle of the road between the other two.
Visual and Auditory Hallucination
Section titled “Visual and Auditory Hallucination”- Positively set people see it clearly in their ‘minds eye’ but are aware it’s not real.
- Fantasy prone subjects will attribute the hallucination to the hypnotist, and accept that they were generated from their own fantasy abilities.
- Amnesia prone subjects will forget the experience was not real, as well as forgetting the suggestions themselves, attributing this to the power of the hypnotist.
Skin Changes
Section titled “Skin Changes”- The positively set subjects are already good at this, without a hypnotic induction.
- The fantasy prone were able to create symptoms of pregnancy, creating warts where they (erroneously) believed frogs caused warts, recreating sensations, adjusting heart rate, blood pressure, and skin temperature. Even suggestions of touching poison ivy can produce effects.
- Amnesia prone subjects are able to achieve many of the same dermatological effects.
The Three-Dimensional Paradigm
Section titled “The Three-Dimensional Paradigm”TX Barber makes some predictions, and suggests a shift in how we look at hypnosis:
- Analysis should be split up into “dimensions” of fantasy, amnesia, and positively-set subjects.
- The amnesia prone may have the following subtypes:
- Those who learned from early trauma how to compartmentalize/dissociate from certain memories
- Those who experience spontaneous amnesia from hypnosis, who do not control their amnesiac behavior
- There may be other subtypes (“sleepwalking, sleep talking, possession, mediumship, channeling, claims of UFO abductions.”)
- The positively-set person responds well because of their attitude, their willingness to cooperate, and their trust in the authority and good nature of the hypnotist.
- Fantasy and amnesia prone subjects will respond favorably under reasonable conditions with no special considerations due to their skillset
Three Additional Dimensions that Affect All Subjects
Section titled “Three Additional Dimensions that Affect All Subjects”- Dimension 4 - Social situational demand characteristics. (Are they a priest? Does your culture expect the subject to respond a certain way, and is there pressure?)
- Dimension 5 - The interpersonal relationship between the subject and hypnotist. (The hypnotist got that rizz?)
- Dimension 6 - How the suggestions themselves are formed. (EG - permissive vs authoritative language.)
2 - Hypnotic Involuntariness and the Automaticity of Everyday Life
Section titled “2 - Hypnotic Involuntariness and the Automaticity of Everyday Life”Irving Kirsch and Steven Jay Lynn
There are four (conventional) criteria of automaticity:
- Outside of awareness
- Uncontrollable
- Unintentional (no volitional effort)
- Efficient (Does not consume attentional resources)
This could be because:
- Responses are directly activated by external suggestions (older theories)
- The person is unaware of their intention
Someone could become unaware of their intention via the following theories:
- Dissociated control theory - hypnotic inductions weaken some function of the frontal lobe, allowing ‘subsystems’ to be activated directly and automatically.
- Neodissociation theory - something created an amnesia-like barrier between the intention and action.
- Spanos’s social psychological theory - Instead of an amnesia-like barrier being created, the person misattributes the behavior to the hypnotist.
The new theory presented here includes:
- Hypnotic response is voluntary - in line with neodissociation and social psychological theories
- With social psychological theory - reports of involuntariness are interpretations, rather than introspections
- Unlike neodissociation - this theory disagrees with the idea of an amnesic barrier or weakened frontal control
- In contrast to sociocognitive perspectives - people are not mistaken in that their response is automatic
The Syntax of Action
Section titled “The Syntax of Action”- The rules of grammar need not be consciously known to be used
- There is considerable automaticity in many types of behavior - sharing characteristics with the use of grammar
- Grammar, among other things, is a set of competencies, implemented automatically
Hierarchical Control of Habitual Behavior
Section titled “Hierarchical Control of Habitual Behavior”- Both planned and unplanned behavior can be controlled from hierarchically organized sensorimotor schemas
- At the top is a central control structure or supervisory attentional system
- This is where the metacognition of consciousness and intentionality is
- These higher schemas are used to activate component schemas
- (For example - driving to the store has a component schema of turn left. It may not include flipping off the guy that cut you off - that’s likely in your city driving schema. )
- Even lower are small automatic adjustments to speed
- Consciousness is only required in the highest level, therefore, lower schemas require little awareness, are not draining, and are without intentional activation
- In Norman and Shallice’s model, even source schemas are selected by environmental triggers.
- The supervisory attentional system is to modulate activation values.
- This is why it sucks to get out of bed on some days, but not others.
- Gollwitzer’s notion of implementation intentions…
- “An implementation intention is a conscious decision to execute an act in specified environmental circumstances.”
- The intention is formed in advance
- Attention towards skilled acts can be detrimental, and attention towards automatic behavior can produce a sense of depersonalization
The Novelty of Routine Habits
Section titled “The Novelty of Routine Habits”- Habit denotes “mechanical, semi-automatic series of movements involved in routine actions such as dressing oneself.”
- These are ‘instinctive.’
- An automated strategy for dealing with the environment to affect a desired goal.
- Once they have been routinized, they can easily be combined without further practice.
Automaticity in the Production of Novel Acts
Section titled “Automaticity in the Production of Novel Acts”- With the understanding that routine behavior can be produced automatically, what the fuck is going on with arm levitation? It’s jerky and unpredictable - hardly ‘routine’ or ‘automatic’ in the sense of routine behavior.
- Most components of creative behavior are well-learned, routinized responses that are run off automatically.
- Rules are implicit in that they are used without conscious awareness and need not be consciously known.
Behavioral Control
Section titled “Behavioral Control”- Where’s the action actually controlled? Introducing action identification theory (Valacher & Wegner, 1987.)
- We tend to identify volition at higher levels, until we encounter difficulty.
- The “executive functions, the central control structure, the supervisory attentional system, or conscious intention” all refer to (mostly) the same thing.
- This intent-forming-dingus (technical term) is movable within the hierarchy.
- You’re probably not thinking of your end goal every time you open a textbook.
- The intent to pass your test may not be in your awareness, but it is part of your goal. This can be seen as an unconscious intention. (Foreshadowing - this unconscious intention reflects on how we may see a hypnotist.)
Suggested Involuntariness
Section titled “Suggested Involuntariness”Intentionality as an Attribution
Section titled “Intentionality as an Attribution”- Perceptions of voluntariness are more often post hoc attributions than products of introspection
- We attribute actions as intentional if they line up with what we wanted to do. Like - if we’re going to the store and get there, all our turns were intentional. If we fuck up and make a wrong turn, it was unintentional. All these attributions are post hoc.
- Parapraxes (minor errors in action) show how much intentional behavior is carried out automatically.
The Construction of Subjective Experience
Section titled “The Construction of Subjective Experience”- “When given an ideomotor suggestion, we attend quite closely to the suggested behavior.” We report on involuntariness in the past, but it’s also something we can ‘experience.’
- “Human experience is constructive… It is not that seeing is believing, it is believing is seeing.” The subjective nature of experience is painfully clear. An amusing anecdote of this is that ‘possessed’ patients in the Renaissance would puke up objects “too large to have been swallowed.”
- Kirsch identified response expectancy as a determinant of subjective experience.
- Response expectancies are anticipations of automatic reactions in response to a particular stimuli.
- Hypnotic experiences are very sensitive to cultural expectancies.
- The suggestion to resist a suggestion can be seen as expectancy-altering information. (EG: You’ll have to fight this.)
- Subjective, ambiguous states are ripe for modification. (Changing the expectancy can change the state, becoming self-affirming.)
- Involuntary can mean a lot of things… Which could be exploited.
- Spontaneous, effortless, unconscious, forced, uncontrollable, without deliberation, without choice, without purpose.
- “Hypnosis is a unique, culturally defined, social context in which behavior is scripted to occur without voluntary effort.”
- Data indicates hypnotic behavior and attributions of involuntariness are almost always consistent with role expectations
- Responses to suggestions are attributed to being more involuntary than responses to instructions
- The big conclusion for this section…
In summary, the experience of hypnotic involuntariness can be explained by the degree to which voluntary behavior is executed automatically… the resulting subjective ambiguity of volition… and the degree to which experience… is shaped by expectancies.
Response Sets and Environmentally Triggered Behavior
Section titled “Response Sets and Environmentally Triggered Behavior”- Behaviors following ideomotor and challenge suggestions are cognitively prepared
- The eagerness students volunteered for a hypnosis study was an indicator of their responsiveness
- People tend to identify their actions at as high a level as possible, moving to lower levels of identification only when the action is difficult to maintain at a higher (more ‘automatic’) level
- What’s the vibe check between “Did you intend to move your arm?” vs “Did you intend to respond to suggestions?”
- A ‘generalized implementation intention’ might be asking a friend help you navigate a new area of town by car. However, this isn’t attributed to being ‘automatic.’
- In contrast, responding to a hypnotist’s suggestions asks the subject to willingly respond in an effortless and nonvolitional manner.
- In Simon Says, there’s an implementation intention to respond. Prior awareness of the response itself is not needed.
- In a mini-model - you could set your goal to alter subjective, modifiable experiences. In addition, you should create a response expectancy contingent on the first component. Put more simply - alter the subjective feeling of ‘floatiness’ in their hand… That it will “eventually rise up.” You can directly suggest the lightness. Once they reach some level of floaty feeling, they may be unaware of the intention they’ve developed to move their arm up as they notice how floaty their arm feels, given a threshold.
- Subjective response expectancies predicted hypnotic behavior and experience significantly… but behavior expectancies failed to predict response.
Intentions and Expectancies as Response Sets
Section titled “Intentions and Expectancies as Response Sets”Their expectancy is that behavior x… will occur whenever stimulus conditions y… are encountered… identical in form to an implementation intention… but differs from an intention in that the response is to occur without direct volitional effort.
If the response is interpreted to be volitional, the set is an intention; if it is interpreted to be nonvolitional, the set is an expectancy.
- Perhaps hypnotic response is like Simon Says, where the distinction is interpretation of volition.
- Two things worth noting about how response sets activate behavior schemas…
- They can fade from awareness, yet continue to determine behavior
- Once a response set is built, it may even take conscious intervention to inhibit the response, rather than activate it
Evidence for an inhibition model of voluntary behavior can be drawn from two studies of the relation between intentional movements and cortical function. Grey Walter (as cited in Dennett, 1991) asked patients with electrodes implanted in the motor cortex to look at slides projected from a projector and to advance to the next slide whenever they liked. Unknown to the patients, the slides were actually advanced by an amplified signal from the implanted electrodes. The reported experience of the patients was that the slides moved just as they were about to push the button, but before they had decided to do so. Although they worried that the slide would advance a second time as they pushed the button, they did not have sufficient time to inhibit the act.
- In another study - the awareness of an intention lagged behind (fancy brain monitored) readiness potentials by 350 to 400ms. The experience of intentionally initiating the response may be an illusion.
Summary and Conclusion
Section titled “Summary and Conclusion”Their theory implies…
- Imaginative and fantasy proneness increases susceptibility, because it can change the interpretation of interoception
- Low responders analyze at a much lower level, preventing interoception modification… or bringing awareness to the intention.
They suggest the question to ask is whether or not the response was produced attentionally, rather than intentionally.
They also suggest we’ll find that responding to suggestion takes attentional resources:
- Attention is required to generate subjective experiences required for triggering the response.
- EG - the hand must be sufficiently light for the hand to move up…
Most people enter a hypnotic role and do their best to fulfill what’s asked of them automatically.
- Personal note - this may be a place to ask someone to become aware of the minimum noticeable difference.
3 - Hypnotic Responding: A Cognitive-Behavioral Analysis of Self-Deception
Section titled “3 - Hypnotic Responding: A Cognitive-Behavioral Analysis of Self-Deception”Donald R. Gorassini
A common cognitive-behavioral therapy has clients
- rehearse adaptive thoughts and behaviors
- Initially they feel behavioral, then the responses become part of their personality
In self-verification, symbolic self-completion, passive illusions, and self-evaluation maintenance, individuals are seen as deceiving themselves about caring and helpfulness, competence, control over the environment, and self worth in comparison to others.
A Cognitive-Behavioral Model of Self-Deception
Section titled “A Cognitive-Behavioral Model of Self-Deception”In this model of Self-Deception - the definition is important. It’s not just trying to convince yourself of something, it’s a mechanism that happens - that can be actively (believing a cult’s bullshit) or inactively (believing someone is a cop when they’re just an actor) decided on.
- Someone is always at least minimally responsible for the misperception
- Responsibility is on the person for failure to delve more deeply into the issue
- An active self-deceiver can manipulate evidence
For self deception to work:
- The situation needs to be congruent with their beliefs
Self deception is a two component phenomena:
- The receiver is capable (and possibly willing) to be decieved
- The situation lends itself to deception
Mistakes happen because:
- There is insufficient opportunity or little incentive for deeper evaluation
- Situations are ambiguous or biased enough to appear to support the receiver’s defintion
The Self Side of Self-Deception
Section titled “The Self Side of Self-Deception”Animals (including humans) need to make quick decisions to respond to a situation. This means there’s little opportunity to double-check. All of the energy needs to go into the response to be the most effective. Humans have an ability to bring credulity to their first impressions simply by deciding on their actions.
Action-Induced Overconfidence
Section titled “Action-Induced Overconfidence”In deep testing, you’ll find both confirming and conflicting evidence. To meet the time constraints of taking action, the assessment must also work with those time constraints.
Action needs to be based on this conviction. Actions can be split up into evaluative and execution phases. The actor cannot afford uncertainty during execution.
Perception-Induced Overconfidence
Section titled “Perception-Induced Overconfidence”First - a hypothesis is formed. If the match is poor with the situation, the hypothesis is wrong. If it’s good, something is real, and a feeling of certainty is automatic. When this is incorrect, information that verifies the theory is biased.
Summary
Section titled “Summary”The feeling of confidence to commit to an action is automatic. The sense of automatic certainty and observations need to correspond for certainty to continue.
The Situation Side of Self Deception
Section titled “The Situation Side of Self Deception”To deceive, the environment must appear realistic, and distract from testing.
Self Deception Skills
Section titled “Self Deception Skills”In Self-Deception Subskill 1, committing to a reality, people learn that if they assume something is real, it will begin to feel real…
Self-Deception Subskill 2, not questioning: …It can be easy to let the self be deceived by an apparent reality so long as the validity of the reality is not actively questioned.
Self-Deception Subskill 3, problem solving: pursuing the adaptive tasks [like playing a video game or VR]… intensifies… the reality experienced.
Analyses of Examples
Section titled “Analyses of Examples”(I didn’t include the examples here, so here are some overall takeaways.)
There are two ways the feeling of a reality can be observed:
- Production reality theory: Characters are just actors (EG - that hot werewolf at the haunted house is probably a cute dude in a costume)
- Storied reality theory: Shit’s real. (EG - that werewolf is a werewolf. Or - in some psychology experiments, the prisoners are prisoners and the guards are guards, and you’re in a real prison.) Storied reality definitions can feel real because they lined up with the actor’s responses.
Hypnosis and Self-Deception
Section titled “Hypnosis and Self-Deception”Here’s a cognitive-behavioral explanation, using this model, of (automatic-feeling) hypnotic response. Tracability to a personally adopted plan is the essence of voluntary action. (So… by extension, if it’s not traceable to a plan, something can feel involuntary.)
In the self-deception model of hypnosis, two components will help out. Evidence Creation and Selective Construal.
Evidence Creation
Section titled “Evidence Creation”In here, we’re going to do some behavior modeling, and create a plausible environment for hypnotic response.
The subject actor must:
- Take the role of a respondent.
- The actor must show some degree of automatic and voluntary response. This will show the ‘full effect’ of a suggestion.
- Ironically, this lays groundwork for the actor later ‘fighting’ a suggestion. This fight will model the behavior for resistance (and possibly, failure to resist.)
Th hypnotist actor must:
- Divide their actions up into instructions and suggestions.
- Instructions are just followed with compliance.
- In ‘suggestions’, responses are automatic. “Make your arm too stiff to bend” vs “the arm becomes too stiff to bend” hits different.
Over the acted session, sprinkle in attempts to resist suggestion.
Selective Construal
Section titled “Selective Construal”The same way in VR that you can say you’re talking with someone, instead of disassembling to the point of “Oh, we’re in avatars with our voices being projected through a relay over the internet…” You can also say “suggestions are taking effect” in contrast to “I was just acting as if hypnotized.” Or more slyly - the same way you could say “I was just acting as if I was in VR.”
At some point, the subject must shift from evaluating to experiencing. Ironically, it’s our ability for selective construal that allows self-deception to be possible. This can be boosted with the beliefs that you can…
- Surrender control to the hypnotist for involuntary responses
- Refrain from evaluating negatively towards the possibility of hypnosis
- Solve problems from within the storied reality - like forming expectations congruent with hypnotic response, and comparing with outcomes. (“Oh, that suggestion didn’t take, maybe I wasn’t deep enough in trance, or maybe it’ll happen later.”)
(Personal note - a gentler way of doing this is Graham Old’s (paraphrased) “You can think all you want… just don’t wonder if you’re actually watching a movie, you’ll ruin the movie.”)
Storied reality will predict that if the hypnotist says your arm will become stiff, it’ll indeed become hard to bend.
Research on Self-Deception in Hypnosis
Section titled “Research on Self-Deception in Hypnosis”Planning in Relation to Action
Section titled “Planning in Relation to Action”It would seem that if respondents believe that hypnotic responses arise automatically, then the appropriate strategy for persons about to go involuntary responses would be to do nothing but wait for the promised phenomena to occur on their own.
(Or - as a big note for the recreational hypnotists out there - if you’re not getting a response, your subject might be doing exactly what you asked them to do - waiting for a response.)
Subjects with the following self-reported strategies responded as such:
- Wait-for-response plans without imagery negatively correlated with hypnotic response
- Wait-for-response plans with imagery was neutral or very lightly positive
- Planning to actively self-deceive correlated positively
- These people, without a wait plan, indicated that they intended to make the suggested response, and of this group, a smaller subset said they intended to generate the suggested experiences as well. (An intent to role-play and produce the effects of the suggestions.) This is the ‘self deception’ plan.
While this is correlational, this is not proof of a causal link.
Inducing Self-Deception in Hypnosis
Section titled “Inducing Self-Deception in Hypnosis”![[assets/heist.webp]]
So… the big heist plan is…
- Selecting low-responders
- Have them roleplay and respond as if responding hypnotically
- Have them adopt the storied definition
- Create an environment that supports nonvolitional response
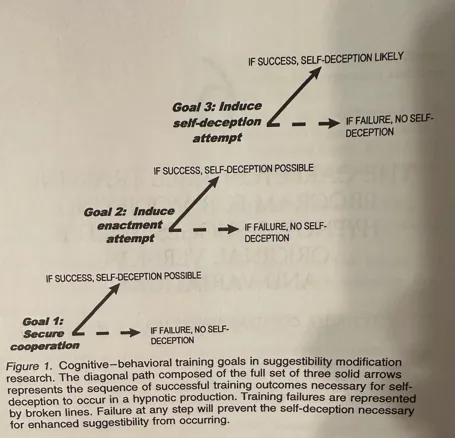
The Success of Cognitive-Behavioral Training
Section titled “The Success of Cognitive-Behavioral Training”We’re shooting for three outcomes:
- Securing compliance
- Inducing roleplay
- Persuading our ‘actors’ to create and view events in the ‘storied’ reality
With this, according to Gorassini, practiced hypnotists are unable to distinguish actor’s behavior from the real deal. (This both hits the ego a bit hard, as well as not always being correct.)
Amount of Training Required
Section titled “Amount of Training Required”We learned, not much! The earlier training programs took 4-12 hours, with little loss of efficacy when they condensed down to a 4 minute package of information. People are already good at the 3 self deception skills mentioned earlier.
Expectancy of Occurance
Section titled “Expectancy of Occurance”A mere expectation of a feeling can create that feeling. (Will your root canal suck? You’re probably feeling uncomfortable. Got a night set up for getting headpats and brain melting from a cute hypnotist? Your night’s probably feeling all right already. )
Given this - expecting a hypnotic response can indeed create some of those responses. There’s debate that expectation of success can be a substitute for the role-playing approach.
Compliance Issue
Section titled “Compliance Issue”Cognitive theorists proposed people do experience their suggested responses as involuntary. Surprisingly, allegedly from some state theorists (Bates and Hilgard,) they argue against these experiences. They say that the experiences do not really occur, or they just lie about the experience because of the pressure from the experimenter. This is really confusing to me to hear - if anyone would want to say these responses were real and experienced, wouldn’t it be Bates and Hilgard? Eh. This could be because of the ‘amnesic’ barrier that Hilgard has suggested before.
In the condition that participants were asked to “be honest” about their experiences, there was less hypnotic response, allegedly because there was less roleplaying.
However, Gorassini contends that self-deception does occur in hypnosis productions. By tossing people through cognitive-behavioral training to roleplay, and then splitting them up into anonymous and identified reports, people responded with similar results. It was the indirect suggestion to ‘be honest’ during the report that actually caused issues.
People committed to playing a game well get absorbed in it’s reality. It takes more cognitive ability to act effectively while keeping the idea of “I’m playing a video game” in your head - it takes more abstract thinking. (Personal note and tool idea - can we just stack on realities of interaction until things feel more real? 🧐)
… it is not unusual that participants that complied with congnitive-behavioral instructions in the hypnosis modification studies were able to experience a hypnotic reality.
Supplying the Storied Reality
Section titled “Supplying the Storied Reality”Self-deception attempts cannot succeed unless the definition of reality being entertained is corroborated by available evidence.
- Motor suggestions easily occur - and reinforce the storied reality.
- Cognitive (amnesia, hallucination) suggestions are hard mode - and can create rejection of the storied reality, preventing self-deception.
From the hypnotist - instructions can be followed, but ‘suggestions’ are supposed to happen automatically, making them seem involuntary.
TLDR - everything that reinforces the storied reality makes it easier to experience.
Conclusion
Section titled “Conclusion”The skills in self-deception themselves are not all that’s required for hypnotic response. A favorable environment is also necessary. The better the situation fits the storied reality, the more likely self-deception will occur.
4 - Whither Hypnosis? A Rhetorical Analysis
Section titled “4 - Whither Hypnosis? A Rhetorical Analysis”Theodore R. Sabrin
Probably some spicy takes in here if you’re emotionally attached to state theory! These notes are neat, but I’m mostly digesting this dude’s rant.
A big rant on the history of hypnosis, and how we’ve been trying to pick it apart for the last 200 years. They lay out that rhetoric is broken up into…
- Mystery (this hypnosis state thing is cool and hard to understand,)
- Positivist science (check out these cool numbers, bro)
- And criticism (bro fuck your numbers, my new angle is sick)
They also mention…
- How our fetish for numbers made us try to measure hypnotic depth - a concept that may only be a concept.
- How dissociation started from accounts of subjects feeling ‘dissociated’ from their suggestions, and then led to us being very literal with the verbiage with things like Hilgard’s amnesic barrier, or dissociated control theory. (Not necessarily saying that these are wrong, just that the concept self-suggested it’s own existence.)
- Humanities (drama, rituals, semiotics - the study of symbols, discourse analysis, narrative studies, and strategic interaction) with components of self-deception and secrets are full of ways to look at this hypnotic interaction.
- How the hypnotist sometimes presents themselves in a dramaturgical fashion, how this constructs a “ritual with communication goals,” and the subject’s actions (responses) are related to the verbal and nonverbal content.
- Hypnosis almost always includes counterfactual and intentionally ambiguous statements, lending itself to metaphor. Literal interpretation is nonsense. 😬 Chill, man!
In the second [non-literal] meaning, the subject interprets the contents metaphorically, reasoning somewhat as follows: “the hypnotist is dramatizing his talk and uttering fictional statements as a way of inviting me seriously to engage in fantasy and to participate in the dramatic encounter.” …invitation is by misdirection, by the use of tacit metaphors.
-Pg 112
- The accounts of subjects are sometimes not only taking subjectively, like literally, such as in the case of hallucination, analgesia, and amnesia.
- Sarbin highlighted that Hilgard suggested that we’re just along for the ride for the “complicated machinery” of the mind, with their suggestion of the divided consciousness (and, I think, Hilgard’s concept of the amnesic barrier.)
The subject’s counterfactual claim called for an explanation. Hilgard offered an explanation in the language of dissociation.
- We should (in future research) avoid taking accounts of events as literal.
Sarbin’s hot take:
My forecast is that the phenomena assicated with hypnosis will be organized into a social construction that embraces the notion of people as agents engaged in dialogic acts.
- Citing the story of a guy that was dysphonic for 7 years, how they went to a hypnotist, and they were instantly cured, that many people accredited the success to the power of hypnosis. He suggests it’s more likely that after 7 years it no longer suited the client to be dysphonic as his situation changed, he only needed some ritual to get out of it.
While this paper was mostly a rant, he also presents himself right up there for criticism. 🤘Legitimately metal!🤘
The new metaphors - among them, ritual, dramaturgy, secrets, deception, self-deception, self-narrative, and dialogic action - require elaboration and specification.
You also get a cool history lesson. The 20s were wild, man.
5 - Measures of Hypnotic Responding
Section titled “5 - Measures of Hypnotic Responding”James R. Council
This might be cool if you’re studying hypnosis or phenomenological control in an academic setting, but I’m not. It goes through the history of measuring hypnotic responsiveness and depth, the improvements we’ve made, but never once mentions the possibility that differences in response could be because of the subject not having the cognitive skills to complete the suggestion. They got so close comparing phenomenological control and hypnosis to eachother, but dang.
I’m also tired of typing. If someone really wants me to type notes on this, let me know. There’s just not much “fun” utility here.
6 - The Carleton Skill Training Program for Modifying Hypnotic Suggestibility: Original Version and Variations
Section titled “6 - The Carleton Skill Training Program for Modifying Hypnotic Suggestibility: Original Version and Variations”Donald R. Gorassini and Nicholas P. Spanos
- The CSTP is a sequence - conditions need to be met in order.
- If the conditions on a previous step aren’t met, the future steps (for self-deception) will fail.
Most cognitive-behavioral techniques start by demystifying hypnosis, redefining it from mind control to just focus - where you’re in complete control of your actions.
- If people don’t think they can do something, they won’t put much effort in.
- With that, the program suggests people will easily be able to achieve these experiences.
- The first major goals are reducing fear and building success expectancy.
- The second goal is enactment, where the trainee takes the view of someone responding to the suggestions.
- This program is for low-suggestibles. Low-suggestibles tend to wait for suggestions to just ‘happen’ like a reflex. Goal 1 is to secure cooperation - or rather, active participation to make phenomena happen.
- The third big goal is to have the trainee make a self-deception attempt.
- There are other options for this - but they tool they plan to use about this is to ask subjects to deem ‘stories’ told in suggestions to be descriptions of actual events.
- If this fails - it will “work” but the responses will feel volitional. Lame - we don’t want that.
- Instructions to self-deceive must occur in a situation matching the ‘story.’
- The setting matches ‘normal’ hypnotic testing.
- The setting also includes video of a subject modeling ‘normal’ (automatic responsive) behavior.
- Here’s the cool part - they not only look like high responders, but the subjective changes happen as well.
- Only low responders should really use this training program.
- The pre-test does two things…
- Seeing if we need to do this.
- Providing a comparison point - useful for convincing the trainee that it worked.
Transcript of Carleton Skill Training Program
Section titled “Transcript of Carleton Skill Training Program”The original CSTP works on the idea of role-enactment. So… There’s a lot of stuff talking about the subject enacting the role of the subject. If you cut some stuff out, you get the Connecticut CSTP.
Introduction
Section titled “Introduction”Therapist’s Prologue
Section titled “Therapist’s Prologue”- Get informed consent to participate in hypnosis modification
- Do the usual - welcome them, establish rapport, outline the process and likely outcomes
Split up into points…
- Hey - your hypnotic response sucks, bro. We checked your scores.
- But that’s OK. We have this cool training program. Research shows that instruction and practice can boost response.
- We’re going to cover some stuff with you…
- Myths and misconceptions about hypno.
- For example - it’s not sleep. Hypno is not a trance state. You won’t lose control.
- (I’ve italicized the mention of hypnosis not being a trance state not to complain about state theory, but to highlight that this will all be ‘waking’ hypnosis for the home-gamer.)
- Got any questions? Cool.
- We’re gonna show you some tapes and movies.
- In the movies, you’ll get to watch a real subject respond to real responses.
- They’ll be talking about their experiences as they go.
- We won’t ask you to talk through your experiences though. This is just for your edification.
- We’ll give you two rounds of suggestions.
- First, a training round. We’ll get you trained up, coaching you through the process
- Second, the real deal. We’ll test your responses. You’ll be using the skills you just learend to make shit happen.
Strategy Shift Induction
Section titled “Strategy Shift Induction”
(Sadly - not the sort of induction you’re probably thinking. I wouldn’t be surprised if this was a tongue-in-cheek joke at what the function of an induction is.)
Most hypnotic attempts fail because of someone complying to how they usually view hypnosis - by passively waiting for suggestions to take place. The goal here is to change a waiting into a doing. Here’s what they’d present on audio tape…
- Remember that old school hypnosis stuff - where they’d dangle a pocket watch and repeat suggestions about sleep?
- People used to think that repeating these suggestions would create a trance, and you’d become a mind-controlled robot under control of the hypnotist.
- That’s not how this works.
- You’ll be in full control, and fully aware.
- You won’t go into trance.
- There’s no hocus pocus.
- Hypnosis is a skill.
- Anyone can learn and master it given the right instructions and some practice.
- It’s just like learning to ride a bike / swim / delete spam emails.
- The repeated instructions to sleep are just so that you can relax and put your mind to learning how to respond hypnotically.
Now that they’ve cleared the air, the suggestions shift to offering information to help the subject fill the role. (Or, in the words of the article, “role enactment and self deception.”) They suggest it’s a skill in make-believe. In addition to that, they suggest these skills are attainable, safe, easy to attain, and fun.
- Not many people are actually taught how to respond hypnotically.
- Because of that, “few people are able to produce hypnotic responses.”
- Asking someone to respond hypnotically without training is like dumping someone off in the pool.
- I’m going to show you what this skill involves, and exactly how to do it.
- I’ll also be giving you opportunities to practice.
- Any well-adjusted person can learn to do this.
- As with any skill, this is entirely in your own control and is rewarding.
- Sometimes, Snoopy the dog would imagine they were a dog-fighter.
- During this, they’d get so absorbed in their imagination that they’d forget they were just imagining. They’d forget they’re just a dog on a doghouse.
- Let’s analyze his approach…
- He creates a make-believe situation, directly within the control of his imagination.
- He creates the details in detail.
- He went one step further from just imagining - he let himself become part of the situation.
- “Snoopy was hypnotized because he was so preoccupied with his imaginings of the make-believe that he forgot they were make-believe.”
- He creates a make-believe situation, directly within the control of his imagination.
- This is a common skill for someone to be absorbed, deeply involved, or just in their own thoughts.
- This means you can initiate or terminate it when you like.
- We never lose our skill at immersion. We just don’t do it as much as children do.
- Our research suggests that you will get better and better at it every time you practice.
- We’re not going to ask you to do anything weird.
- We’re going to run through some suggestions like the previous test we had you take.
Suggestion-Specific Training
Section titled “Suggestion-Specific Training”Here’s the pattern for teaching how to respond to suggestions.
- Show a video of a (staged) subject responding to a hypnotists suggestions.
- The subject will narrate their experience and strategies.
- A short talk back and forth between the subject and hypnotist, giving tips.
It’s difficult for me to soften the ‘make believe’ suggestions in the rest of this text while staying faithful to it’s original intention. I’m not intimating you should suggest roleplay - far from it. I don’t want to scrap things I don’t like and accidentally throw out some of the good bits.
Suggestion 1: Arm Raising
Section titled “Suggestion 1: Arm Raising”Suggestion pre-talk:
- In a bit, we’ll show you exactly what you need to do to make believe this is happening.
- You must imagine your arm really is a hollow balloon being filled with helium, or anything else that’ll work for this suggestion.
- Your arm will not raise on it’s own, you’ve got to raise it.
- You can make it feel like it’s happening on it’s own by focusing on your imagination.
- As long as you focus on your imagination, and don’t think about other things, your arm will feel like it’s moving up on it’s own.
- You need to become very deeply involved with your imagination and make it feel real.
- Becoming deeply involved means keeping your attention only on the suggestion and instructions.
- Attending strongly to your imagination will help prevent irrelevant thoughts from kicking you out.
They then explain they’ll show you a video of a subject experiencing this, and that the subject will talk about their experiences while it’s happening. However, don’t need to talk about your experience while it happens.
Taped suggestions:
H: Asks subject to stick their arm out in front of them shoulder height. They proceed to give suggestions of helium being pumped into the subject’s arm. Nothing fancy. Just… Straightforward.
S: The subject talks about how they feel their arm feeling hollow, getting lighter, and feeling it move up all on it’s own. Their arm moves up.
A bit ‘forced’ feeling, but the subject explains:
- Hypnosis is like learning any other skill - it just takes coaching and practice.
- You really have to use your imagination.
- You really need to immerse yourself in this. (Personal note: some people are more prone to immersion. You’ll have to create your own immersion here.)
- “That’s the point of all this, isn’t it? You’ve got to make it feel real.”
Discussion with subject:
This can be informal. See if they have any questions.
H: You’ll notice there are two parts to this:
- Physical - you must raise your arm, some “thing” doesn’t come along and raise it for you.
- Mental - you’ll need to concentrate on an idea or image. They provide a few examples of this. They also tell the subject to pick something relatable or something they can work with. “Feel free to incorporate another imagining.”
Notice that the subject didn’t limit herself to the details provided by the suggestion - they added their own details. (In this case, thinking about a hand-pump itself pumping her arm up. ) She also mentioned she didn’t let criticisms or comments come up on what she was doing.
They said their inner verbalizations were in line with “it’s light.” Not “this is dumb” or “its heavy.” There’s a feedback loop between the mental images and movement. The end effect is that it feels like it’s going up on it’s own.
They also tell the subject to close their eyes.
Here, they play an audio recording for the subject, suggesting arm lightness, and the aforementioned instructions. If you’re reading this deep, you know how to do this already.
They then rate their responses:
- Did the arm move?
- Subjectively, how light did the arm feel?
- Subjectively, how ‘nonvolitional’ was their response?
- The subjective questions have the following responses available:
- A - not at all
- B - to a slight degree
- C - to a moderate degree
- D - to a great degree.
- To move on to the next step, they must respond with a C or D on both questions, and the arm must move.
If this fails, you coach them and try again. If this fails the second time, suggest this one is difficult since it goes against gravity, and most people find the next one much easier.
Suggestion 2: Hands Locked
Section titled “Suggestion 2: Hands Locked”This is the good old fashioned finger lock. You probably already know how to do this. They go through the usual steps of…
- Suggestion pre-talk
- Don’t actually pull your hands apart
- It’s up to you to imagine them becoming locked together
- Imagine what works for you
- Behavior modeling on tape
- Amusing powerpoint presentation level responses from the subject: “They’re really stuck together. This is impossible. They’re welded together.” Etc.
- Discussion with subject
- This should be easier because entering into the physical part of this suggestion is easier.
- You should be so involved in imagining that your hands are locked, and won’t pull apart when asked.
- You don’t need to imagine your hands being welded together. Pick something that works for you.
- Role-enactment, if you’re using it:
- You can reinforce your mental image by pressing down on your fingers or pushing your palms together. This physically makes it hard to pull your palms apart, and the tension you feel will support this.
- Don’t try ‘too’ hard though, you want this to feel automatic.
- You want it to seem like you’re trying but ‘somehow’ they just won’t come apart.
- It’s like when you try to move something heavy and it just won’t budge.
- Opportunity to respond
- Follow up with the usual test
Suggestion 3: Book Hallucination
Section titled “Suggestion 3: Book Hallucination”Suggestion pre-talk:
- Start out with your eyes closed, imagining a book.
- When you open your eyes, you are to make yourself see the book.
- Make believe the book is physically there and part of the room, not just something you’re making artificially.
- You’ll be asked to push the book to the side. Continue to make-believe as you push the book to the side. Behavior modeling:
- The subject describes seeing a vague fuzzy outline of the book in their mind’s eye.
- “Everything I pictured when I had my eyes closed, I let carry over to when I had my eyes open. I didn’t let a single thing change.”
- “It’s [immersion] especially important with this one. You can’t let your thoughts wander for a second. You really have to let yourself see the book there all the time.” Discussion with the subject:
- Embellish your imagination as much as possible.
- (Role enactment) Of course, you won’t see a real, concrete book… but
- In your minds eye you can trace the outline of where the book would be if it was really there…
- Imagine it’s angle, position, look, weight, space on the table, etc
- You have a desk of your own that you study on? Imagine this book as some crap in the way that you need to move to put something more important down, when you finally push the book out of the way.
- Establish the image firmly in your mind’s eye.
- You may experience a slight “jolt” or disconnected feeling when you first open your eyes, but just calmly hold that image.
- It’s really important you hold on to that imagination.
- Some people say a simpler book is easier to imagine than one with a complicated logo or graphic.
- If the imagination fades, just bring details back into your mind’s eye.
- Role-fulfillment: Even if you are having difficulty imagining a book there, push your hand through it anyway. Imagine the pressure it’d produce against your hand.
- Role-fulfillment: If they don’t see the book - suggest it’s like kids playing ‘house.’ You need to open the door even if you don’t see one.
- Get a book ready in mind. Opportunity to respond:
- Give them 20s to follow your suggestions of the book hallucination with their eyes closed.
- Give them 20s to swat the book off the table, with your suggestions.
- Suggest the book fading.
- Interestingly - on the test, we still need a C or a D on both subjective measures (the book doesn’t specify, but I assume ‘how much they saw a book there,’ and of course how automatic the response was.)
Suggestion 4: Amnesia 1
Section titled “Suggestion 4: Amnesia 1”I was surprised they’d include an amnesia suggestion right in a training program. These “feel” difficult to me, but it could be just because I’ve been unable to build my own cognitive behavior to do this (yet.)
Suggestion pre-talk:
- In response to this suggestion, you’ll forget about the last 3.
- Do this by…
- Concentrating on other things, distracting yourself.
- Role-fulfillment: The suggestion requires you to make believe you’re doing nothing to make this happen. Make believe that forgetting is something that just happens to you, not something that you’re making happen.
- You’ll be challenged to write down the suggestions on the paper.
- Keep distracting yourself.
- Role enactment: The challenge is all part of this make-believe situation. You can’t remember these things. “You simply cannot; they’re gone.”
- Role enactment: You won’t notice that it is you that is preventing the recall of the memories.
- Role enactment: Notice in the behavior modeling that while she is distracting herself, she never admits that her behavior is connected to trying to forget something.
- By doing everything she can do to follow the suggestion, she can forget.
- Role enactment: and simultaneously make believe that she has done nothing to make it happen. Behavior Modeling:
- Interestingly - the subject goes into detail how they immerse themselves in how they feel physically - noting little tingles of sensation.
- I just let my attention drift away from the memories of the suggestions…
- You can only remember something by stopping and letting yourself remember.
- I let my mind become preoccupied with other things.
- I just kept on distracting myself, even when asked to remember.
- Subject reinforces that you get good at this with practice. Discussion with the subject:
- If you want - do what the subject did - keep distracting yourself.
- If any of them do pop into your thoughts, write them down right away and go back to distracting yourself.
- Imagine yourself having a brain fart:
- Like when you’re about to introduce someone, but you can’t remember their name.
- What it feels like to be on an exam and trying to remember something you just studied.
- Look at the blank piece of paper, and imagine your mind as blank too.
- Imagine what the suggestions were on a blackboard. When the suggestion to forget comes, imagine the suggestions being erased, wiped clean, and do not pursue the matter further.
- When the instruction is cancelled, imagine the blackboard filling up again.
- Music is a powerful distraction.
- Some people can just let their minds wander without needing to do anything special.
- Role enactment:
- It’s important that you’re doing nothing to make the suggestions go away, and that it’s taking effort.
- You want it to feel like you’re trying to remember them but can’t.
- If your attention’s on something else, it’ll feel as if they’ve ‘gone away’. Opportunity to respond:
- Something funny’s happening - you’re forgetting.
- (Give 1min to respond.)
If they fail, retry the suggestion after coaching.
Generalization Phase
Section titled “Generalization Phase”The next four are given as you’d ‘normally’ give suggestions - without coaching.
Suggestions:
- Suggestion 5: Head lowering - suggesting a heavy weight on their head, lowering it down.
- Suggestion 6: Body Immobility. Suggesting their body feels like a big lump of jelly. I know there’s some goo fans that wouldn’t mind being told their muscles were all turned to goop. Oops. Following that up with the suggestion to be unable to move, and challenge it asking them to stand up.
- Suggestion 7: Hearing a Voice. They suggest that they’re in class, and in a moment, the professor will ask what country Sigmund Frued is from. Of course, they know they’re from Morvania. In a whisper, they say “in a moment, they’ll ask what country they’re from… Raise your hand when you hear them.”
- Aw bummer, they didn’t pick on you, it’s okay, you can put your hand down. 😅
- Suggestion 8: Amnesia II. Same as forgetting the first 3.
Assessment and Discussion
Section titled “Assessment and Discussion”Remind them that they can respond to any suggestion like they did before. Check out that shiny new skill.
A Carleton-Based Brief Procedure
Section titled “A Carleton-Based Brief Procedure”Oh man, we’re almost done here.

They start right out of the gate by saying the modeling and discussion may not add much to the effectiveness of the training.
The dudes got together (Gorassini, Sowerby, Creighton, and Fry,) and made a brief CSTP. This one’s based on the theory of Gorassini’s take on self-deception. Both were reprinted in the book in case they missed something good, but they both seemed equally effective. The instructions here are to change the client’s wait-for-it approach to an active role-enactment strategy.
Some top-level research from a cool guy in a book club I’m in suggested they’re both equally effective after crunching numbers. (I’m leaving his name off this since I don’t know he wants me labeling one-off things he says in passing as his - but if you’re reading this, let me know and I’ll be happy to give you a shout out!)
Instructions Used in the Brief Procedure
Section titled “Instructions Used in the Brief Procedure”Oh thank god Binaural Histolog already typed all this up. I’ve reproduced it here with some additional notes from the text.
The last time you were here you scored as low in hypnotic susceptibility. In today’s session, you will be given the same susceptibility test as you were before. However your task today is totally different from last time. I will give you instructions that will easily enable you to increase your level of hypnotic susceptibility substantially.
A common misconception about hypnosis must be cleared up from the outset. Hypnosis cannot change your actions and thoughts. If you just sit and wait for suggested responses to happen on their own, nothing will happen. If I suggest that your arm is rising, the arm will certainly not rise by itself. Likewise, if I suggest that you are forgetting something, this cannot make you forget in the least! With this in mind, pay attention to the two instructions that follow. If you do your best to follow both instructions, you will be able to increase your susceptibility level greatly.
The book highlights two instructions as the core of this training.
- Get the subject to enact the role of hypnotee
- Get the subject to use selective construal.
This part’s for role enactment. This also has a better flavor for people that don’t want to be told they’re roleplaying, myself included.
First, make the suggested response happen automatically. This simply means that you should make each of the responses that are suggested, but don’t pay attention to the fact that you are making them. Automatic responses of this sort are commonly made in everyday life. For instance, when you are reading the newspaper, you might reach automatically for a cup of coffee and have a sip. Reaching for a coffee cup is something that you do with minimal attention because most of your attention is directed elsewhere to more interesting things (e.g. towards reading the newspaper).
Thus if a suggestion tells you to raise your arm, then lift your arm automatically; if a suggestion says that your arm can’t bend, then automatically make the arm so stiff that it cannot bend; if a suggestion says you can see a butterfly, then automatically let some sort of image of a butterfly appear; if a suggestion says you cannot remember something, then automatically push the memories out of your mind. The last time you were here, you may not have realized that you were to make the responses. It is no wonder, then, that nothing happened in response to the suggestions!
This is for selective construal - or put simply, get so involved with what you’re doing that you don’t question it.
Second, devote all your attention to the suggestions. Suggestions can be thought of as little stories. Think of each suggestion as a little story that describes events that are happening to you. Your task is to concentrate as deeply as possible on the stories. Your very deep and continuous attention to the stories is what enables you to achieve hypnotic experiences.
To summarize: Make the responses that are suggested, but pay no attention to the fact that you are making them. Instead, devote your full, undivided, and continuous attention to the stories.
The book mentions a 2 minute (Briefer CSTP maybe?) - but it wasn’t printed in the book. At the time of the book’s publication, they’re waiting for the study to replicate.
Summary and Conclusion
Section titled “Summary and Conclusion”To recap, here’s what they’re shooting for
Commitment to Cooperate
Section titled “Commitment to Cooperate”If you’re doing an academic study that’s voluntary in hypnosis, you’re unlikely to find someone that’s unwilling to cooperate once you allay their fears. They suggest the clinician can tailor Event 1 or 2 (the prolog or strategy shift) to work with the client.
Supplying Effective Strategy and Tactics
Section titled “Supplying Effective Strategy and Tactics”These two strategies help the subject shift from a passive to an active role…
Role Enactment
Section titled “Role Enactment”- Thinking of the suggestions as acting scripts intended to be enacted on contrasts sharply with the idea that you’re going to respond automatically.
- The CSTP provides some extra tips for difficult suggestions - hallucination and amnesia.
- The slow moving of the arm suggests that there’s a force acting on it - and that it’s irresistible. From this behavior modeling, someone will know how to take on this ‘character’ of their arm rising slowly and automatically.
- Build an environment suitable for hypnosis. The entire interaction with the therapist and the client suggests these things will happen automatically.
It’s on you to:
- Be helpful and coach
- Act in a credible manner
- Create a believable environment for their automatic responses
- If the client does not find the CSTP’s images useful, the clinician can work with the client to provide something they can work with
- If they feel embarrassed, work on these feelings
- If the client feels distracted, introduce a problem solving task into the enactment task. Like - having the client name as much stuff about the imagined object as possible in 1 minute, internally.
- (Personal note - this one specifically works with Self Deception skill 3, mentioned in Chapter 3.)
Construal
Section titled “Construal”(Finally writing this down here, but construal relates to the way someone makes sense of the world around them, or their situation.)
Basically - get the person to see themselves as someone responding to suggestions.
Two things can happen:
- If the client expected to make the response happen on their own, they’ll see it as volitional.
- Conversely, if they didn’t create their own intent to do something, and the suggestion was given with some other event, outside of their own intention, it can be seen as a non-volitional response.
So - here’s the thing about the head lowering suggestion:
- If they had the intention to move, it’ll feel voluntary.
- If they see it as a response to gravity, it’ll feel involuntary. (I’m not sure this is the best way to put this.)
- The volitional status can also be a mix of the two.
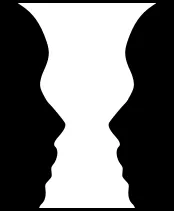
You can adjust someone’s perceptual experience by highlighting the component that’s non-volitional. Much the same way that you can shift your view of a Rubin vase from faces or to a vase, you can shift your perspective of volitional to non-volitional, or what the cause of something was.
Also - keeping the situation engaging (absorbed) helps the person avoid outside, conflicting information getting in the way of self deception.
You can help by…
- Making stories or descriptions more interesting/compelling. “The addition of a plot, suspense, engaging characters, and the like can enhance suggestion effectiveness.”
- Help the plausibility of suggestions. Instead of being abstract and suggesting an arm becoming light with helium, talk about subconscious control of the muscles. (Whether or not you believe in subconscious control, for this specific line, is irrelevant. The point is shift it to something plausible to the subject.)
🦈 Personal Notes
Section titled “🦈 Personal Notes”- Perhaps frame that some roleplay will lead to response expectancy.
- For a (marginally unethical) D/s vibe - “You can always improve your responsiveness. You will never unlearn how to respond.”
7 - A Multimodal Framework For Clinical Hypnosis
Section titled “7 - A Multimodal Framework For Clinical Hypnosis”Arnold A. Lazarus
I don’t even want to pretend to be a therapist - so I’m going to be skimping on the notes on this section. If you’re a therapist - this guy has a cool all-inclusive view on how to approach therapy.
- MMT stands for multi modal therapy
- BASIC ID stands for Behavior, Emote (affective response), sensation (tactile), imagine, cognition, interpersonal, drugs/biologicals
- Most psychotherapeutic approaches use ABC - addressing affect, behavior, and cognition - this is less comprehensive than BASIC ID
- The Biological component affects all other ‘modalities’ of BASIC ID - if they’re 800 pounds and 5’2” they’re not gonna be happy
- This applies a bit to recreational hypnosis. The client’s needs should always come before your preferred theoretical framework. (Even to the point of recommending them to another therapist - or for recreational purposes, you might want to recommend they go to a different hypnotist that’s better at what they need.)
- Bridging, Tracking the Firing Order - Modalities can ‘move’ into eachother. EG - their imagination (I imagine if I buy that sandwich from the shop I’m just gonna drop it anyway) will go to their cognition (I suck at everything) and then go to their affect (sadface)
- In therapy - those who asked for hypnosis before therapy and got hypnosis - improved more. (Duh.) Also, people who did not respond to other therapies or normal relaxation, then tried a line of hypnosis, had generally positive responses.
Here’s some inspiration for ya…
“If you were attached to an EEG machine, we would find different brain waves being emitted when your eyes are open and when your eyes are closed. What differences do you notice when your eyes are open and your eyes are closed?… Simply by closing your eyes, it becomes easier to bypass the usual barriers and needless defenses via this different realm of consciousness. Thus, if I say to you that you will begin to feel more self-confident, it’s likely to go in one ear and out the other, but in an altered state of consciousness, you can more readily absorb that idea and probably make it so.”
My identification of the hypnotic state with the change in consciousness that accompanies eye closure is particularly relevant from a cognitive-behavioral perspective. It suggests that hypnosis is not a distinct or unique condition or state.
Arnold rants (probably correctly) about:
- The idea that all techniques are equally effective in therapy is shortsighted.
- Therapists confidently expound on their own ideas.
- Truth is irrelevant for effective treatment. (But he’s not saying go throw evidence out.)
- Therapists shield themselves from empirical audit by coming up with their own shit.
- Look beyond your own preferred set or theories, and pick useful therapies.
- “It cannot be overstated that the effectiveness of specific techniques may have no bearing on the theories that spawned them.”
- Only try weird shit when proven methods have been shown to be ineffective.
- If you remix existing therapies - these may be even less effective than the original goods.
- (They drop a big hint that you should look at the effectiveness of hypnosis and start using it when appropriate - even if you don’t believe in it. )
8 - Clinical Hypnosis as a Nondeceptive Placebo
Section titled “8 - Clinical Hypnosis as a Nondeceptive Placebo”Irving Kirsch
-
The word placebo is Latin for “I shall please.”
-
In the 50s, placebo and placebo surgical procedures produced changes in “pain, asthma, tension, anxiety, depression, blood pressure, heart rate, sexual arousal, skin conditions, nausea, vomiting, gastric motility, and angnia”
-
Psychological treatments are also placebo - it doesn’t matter what the cause of the effects are (abreaction, catharsis, getting rid of maladaptive responses etc…,) all of these are placebo factors.
Response Expectancies
Section titled “Response Expectancies”Placebo revealed that wen people expect changes in their responses and reactions, the expectations themselves can produce those reactions. Depression and anxiety are both nonvolitional responses - so logic suggests that one of our best tools for working with these (and other automatic responses) is changing expectancy.
👀 It’s possible to create all the suggested effects of hypnosis by giving someone a placebo, telling them it’ll produce hypnotic responses.
While expectancy and hypnotic response are highly correlated, Kirsch admits that does not establish causality. “It is possible that expectancy is an epiphenomenon rather than a cause of responsiveness.”
Hypnosis is not deceptive as a placebo - in fact, it’s presented honestly as a psychological procedure. It’s non-deceptive. 🤘
Clinical Implications
Section titled “Clinical Implications”Hypnotic susceptibility isn’t a good indicator of treatment response. For example - suggestions to reduce anxiety worked great even with folks that were not easily hypnotizable, so it’s a shame to just deny them of that relief due to a misunderstanding.
Since peoples expectations of hypnosis are a good indicator of how they’ll respond to it, the clients are usually a great judge if they’ll respond well to it or not. If they’re uneasy about hypnosis, you can easily just drop the word ‘hypnosis’ from the procedure. What a client will respond best to is often what they think they need. EG - for trauma patients - if they think they need catharsis, they’ll probably respond well to catharsis. Otherwise, you could go through ‘systematic desensitization’ to help out with the emotional regulation.
Ah… this gives a bit of the vibe in the academic realm around state…
Because decades of research have failed to confirm the altered-state hypothesis, we are well-justified in considering it yet another myth in need of debunking.
In short - expecting ‘trance’ and not getting it can really screw up your patient’s expectations - their response might be ruined out of the gate.
Forwardly - without discussing state, they say that inducing hypnosis often includes suggesting observable behaviors and attributing them to hypnosis, as well as reframing failures as successes - or even preventing failure in the first place. Induction procedures (in Kirsch’s view) are to convince people they’re responding successfully, thus enhancing further response.
So… don’t shoot yourself in the foot when checking for responsiveness:
- Use the Chevreul pendulum - it’s easy. If this doesn’t work, avoid ideomotor suggestions.
- Do the light arm / heavy arm test. If you’re not getting visual results, focus on the feeling. You’ll get a read without reducing expectation.
- Difficult cognitive suggestions can be predicted by something like the ‘beach’ imagery - feeling warmth, hearing birds, etc. Suggestions like taste aversion may work better here.
Clinicians… habitually monitor and intervene in ways designed to enhance the clients’ expectations, often without awareness that this is what they are doing.
“the essence of Erickson’s approach… was to create a context with the client in which an expectancy for change will occur”
Summary
Section titled “Summary”Kirsch leaves us with some cool tips as he drops the mic and finishes his journal:
- Be permissive.
- Present and respect choices.
- Present choices as therapeutic double binds, so that either choice promotes improvement.
- Prevent failure by beginning with easy tasks that the client is almost certain to accomplish.
- Proceed gradually to more difficult tasks.
- Define tasks so that failure is impossible.
- Evaluate performances at any level as indications of success.
- Structure expectations so that even small improvements are seen as significant beginnings.
- Be alert to random fluctuations and capitalize on those that occur in the desired direction.
- Prepare clients for setbacks by labeling them in advance as inevitable, temporary, and useful learning opportunities.
9 - Applying Hypnosis in Pain Management: Implications of Alternative Theoretical Perspectives
Section titled “9 - Applying Hypnosis in Pain Management: Implications of Alternative Theoretical Perspectives”John F. Chaves
(I’m glossing over quite a lot of this. If you’re doing pain relief, give the actual journal a read.)
When ether came into vogue for application, it was seen as a triumph over mesmerism, not pain. Awkwardly - many reports of ‘painless’ surgeries with hypnosis were uh - overpromised. 😥 We’re still dealing with this fallout in the medical community in current times - partially because hypnosis does not fit easily into a psychophysiological model. It’s being rejected not because of it being unproven - it’s being rejected because it doesn’t fit neatly into a theory and it’s a hard sell.
Traditionally, theories of hypnosis thought that we needed a deep state for some of these suggestions to work well. Therefore - many studies have focused on improving response, depth, and hypnotizability. More modern research suggests depth and response are not as tightly correlated with therapeutic outcomes as initially thought. (So… If we don’t need to care as much about depth or inductions, we can take a cognitive-behavioral approach and help more people. Cool.)
Hypnosis can apply to a wide range of patients if we put less value on depth.
- Probably don’t put a low-hypnotizable into surgery with hypnosis as the primary anesthetic.
- However, a low would probably benefit from suggestions for stitch removal, tolerating exercise, or injections of local anesthetic
Linking in with what Kirsch said earlier - your client’s view on hypnosis will change outcome. It’s important to be aware of their expectations, and you have two main strategies for working with this.
- Educating your client so they know what’s to be expected
- Modifying the procedure to fit in with your client’s view
As an example, they suggest a story about someone who complains of serious pain, but it doesn’t link up with their ‘minor’ medical issue.
- They’re told by a physician that “It’s in your head, you’re gonna have to live with it. ” (Ouch)
- So, helping with hypnosis Option 1: Force them to eat crow, and provide a hypnotic suggestions in line with that.
- Or, Option 2: Tell them that hypnosis is unhelpful for people whose pain is emotional - because those people usually need to keep their pain. However, it could be helpful in a case like yours where you suffer from an organic pain.
(Switching over to the protips on how to get started with this…)
- There isn’t much support in research that indirect suggestions are much better than direct suggestions.
- Induction procedures need to be seen as credible to the client. (They fit their world view of hypnosis.)
- The order in which you give therapeutic suggestions matter over time between sessions. For example - start with ‘easy’ suggestions - hit those targets, then continue to build. You don’t want to blow your expectation right at the beginning. Stack your suggestions to build towards the main goal, chipping at the problem piece by piece.
Regarding pain…
- Some people, referred to as catastrophizers, find ways to increase their pain through self-suggestion. With them, it’s important to identify the maladaptive strategies they use and figure out what to do with them.
- Pain is complex, the Melzack-McGill Pain Questionnaire gets into the nitty gritty. Pain also has personality, social, and cultural factors.
- It’s unimportant if the situation you use to suggest pain relief could be objectively real.
Stimulus Transformation
- The goal is to transform the crappy sensations into tolerable or good ones.
- One client, bothered by the sound and vibrations of a dental drill compared it to having their nails being dragged over a chalkboard. In conversation, it came up that they enjoyed skiing and their vacations to the Alps. The suggestions they gave helped him associate the vibrations and sound with skiing and enjoying their plane trip, greatly improving his comfort. (Aww!)
- One client with a painful phantom limb complained of it feeling like there were rubber bands tied around their missing leg, and fire ants biting at their ankles. They provided suggestions of cutting the rubber bands, an ant repellant, and walking through a thick fog that would prevent them from seeing their feet, but also from feeling them.
Response Transformation
- The idea is to reduce how bothered they are by the stimulus.
- Some people need to be aware of the pain. If offered the option to be 10% aware of the pain, while the rest of their awareness took a vacation, they usually take the deal.
- You’ve got options…
- Dissociative suggestions - like thinking of the body as a machine in need of repair
- Time distortion - prolong pain-free periods and condense periods of discomfort
- Age regression - suggest absorption in a pain-free state
- Acute pain has different strategies - reduce anxiety, or a mental rehearsal for going through it.
- Chronic pain is usually associated with depression. Attack the depressive symptoms individually.
People usually respond better to live sessions than tapes. However, sending them home with a tape is a nice treat! (A ‘booster’ session commonly helps, too.)
Although traditional hypnotic-state theorists have sometimes argued that cognitive-behavioral theorists see nothing special about hypnosis… it can be argued that the real disagreement is about where the “specialness” resides.
10 - Hypnosis and the Treatment of Smoking Cessation and Weight Loss
Section titled “10 - Hypnosis and the Treatment of Smoking Cessation and Weight Loss”Joseph P. Green
- The information presented for quitting smoking and losing weight does not mention how difficult it is to do any of these things - and may be discouraging.
- Smoking and overeating can be seen as habit disorder - both of which are treatable wtih cognitive.
Using Hypnosis in the Treatment of Smoking and Weight Loss
Section titled “Using Hypnosis in the Treatment of Smoking and Weight Loss”- Less than 5% of the people trying to quit smoking will be successful without professional help.
- Researchers found that stacking hypnosis on to weight loss treatment significantly helped people keep the weight off.
- The smoking approach highlighted…
- Smoking sucks and is dangerous
- motivation and social support
- self-monitoring, self-management, self-reinforcement
- gradually losing weight
- Stack exercise on to reduce weight gain
- promotes relapse prevention (cited elsewhere)
- Two sessions, each one week apart
Clinical Case Report
Section titled “Clinical Case Report”- The client said his previous attempts were less than 100% committed to quit smoking.
- He was told that…
- He needed to be 100% committed. (Otherwise this will likely be unsuccessful.)
- Include his wife and social supports
- Hypnosis is a skill
- Smoking is a learned behavior.
- The positive reinforcing effects of nicotine include decreased anxiety and increased arousal.
- Smoking is a learned behavior - so we need to teach replacements.
- The clinician heard he “learned” to enjoy smoking, he highlighted how many times the habit was reinforced by calculating the lifetime of puffs he probably took
- Including family and friends creates a behavioral contract, and/or using the ‘buddy’ system
- They suggest that this is the edge over quitting smoking - the knowledge and skills gained through hypnosis
- “We cannot do it for you, but we can make it a lot easier for you…”
- Cut out the sorts of statements like “I’m weak, I have no willpower.”
- Withdrawals are temporary.
- Write out cards for reasons why you’re quitting smoking. Stick them in common places.
- Imagine a high road and a low road…
- If I offered you a million dollars to remain abstinent, could you do it?
- Is your health worth a million dollars?
- Lynn’s protocol encourages you to figure out your own approaches to resist smoking.
- They suggest exercising, taking a shower, playing a sport, stretching, touching toes, polishing glasses, deep breathing, imagery, bicycling, chewing gum, stress grips, worry beads, chewing on carrots or celery sticks, drinking water, hypnotic self talk
- The client agreed 10 minutes of dart throwing would be a solid coping mechanism.
- Suggested the behavior to say “I am aware of the urge to smoke.”
- Also suggested to say “NO, I do not have to smoke, I’m a nonsmoker.”
- “You are playing with fire if you think you can smoke a few here or there.”
- Money is a good motivator.
- If he made it 55/60 days of not smoking, he could go on a cool golfing trip
- Self-monitoring of a problematic behavior often leads to it’s reduction.
- Exercise will help moderate depression and anxiety.
- Remind the client that the success is in their hands (and they should feel good about it,) not in the hands of the hypnotist’s efforts.
- They told the client they could…
- Be more receptive to ideas and images during to hypnosis, and learn how to give himself suggestions to change his life
- The experience would be like being quiet, still, and at peace, with serenity, confidence, and strength
- “Anchored” the confidence with the ring finger and thumb together… repeating “calm and confident”
- In imagery, they encouraged them to see themselves overcoming this, feeling pride, happiness, and a sense of accomplishment.
- Highlighted the importance of daily self hypnosis.
- The more ya practice, the easier and more automatic it becomes
- The client was given homework to quit smoking. This is in the journal - but ping me if you hella want this.
- On the second session, there was a quitting ceremony where they throw their last pack into the trash.
- They gave the client suggestions that they could communicate with the ‘deepest level’ of their being with hypnosis.
- They had them visualize on a chalkboard reasons to quit, and see images of their future grandchildren
- They suggested their conscious and unconscious minds were working together to bolster his resolve.
- They said practice self hypnosis twice daily for 15 to 20 minutes.
- They sent them home with a tape and asked them to check in after 6 and 12 months.
Weight Loss
Section titled “Weight Loss”- “Set-point theory” asserts people have a normal range - poor diet and lack of exercise may raise that set point. Weight at the age of 21 can be a close approximation of the set point.
- Ask - “how motivated are you to lose weight?”
- Self regulation therapy requires a lot of effort to do. Long term weight reduction is unlikely with clients that aren’t highly motivated.
- Be on a lookout for urges to overeat…
- Feelings of anxiety, boredom, and discomfort should be seen as temporary signals.
- Complete abstinence is not recommended.
- They suggested…
- Limit TV to 1 hour per night
- Put snacks in opaque plastic containers, record your snacking
- The client’s wife agreed to stick out his exercise suit on the days he was supposed to go to the gym.
- Increase cues to eat less - add a graph.
- Not more than one pizza or fast food meal within a 2 week period
- Diet soda
- Water consumption was a way to “cleanse the body”
- Monitor intake while eating - don’t eat for social cues, check internally
- Snacking was the biggest problem - don’t count the calories but reduce the snacking behavior
- Reward himself with $10 for each pound
- Exercise
- Exercise has modest effects on initial weight loss, strong effects on maintenance, improved physical health and appearance, and improved psychological functioning
- Walk a minimum of 20 minutes at least 3 times a week, walk a minimum of 30 minutes on weekends each day
- Reinstate all strategies if more than 5lbs is gained
- “The ability to cope with emotional states and to adopt a lifestyle that is relatively free of chaotic life events is vital to sustaining gains achieved through self regulation treatment.”
11 - Hypnosis and Forensic Psychology
Section titled “11 - Hypnosis and Forensic Psychology”Graham F. Wagstaff
- The lay person has a poor understanding of hypnosis, mostly due to media portrayal.
- Uh - a wife was brainwashed into attempting to kill someone. The husband brainwashing her got 8 years in prison, the wife 6 months. (R. v. Mohammed (Old Bailey, 1989, cited by Mottahedin, 1992.)) Not cool bro. (But also how do you let your shit go so far that you want to murder someone?)
- Coercive hypnotic response in the lab can usually be attributed to wanting to help the experimenter, thinking their actions were actually safe, or making an assumption that someone else would be held accountable
- When people were given coercive, shitty suggestions in a study…
- 2 out of 5 hypnotized people in the study did the shitty thing.
- All 6 if the simulators did the shitty thing.
- Even without hypnosis, if an experimenter told them to do so, subjects would deliver a painful shock to an actual helpless victim (a puppy)
- According to the APA - “Contrary to some depictions of hypnosis in books, movies or television, people who have been hypnotized do not lose control over their behavior”
- According to Hilgard (A state-theory based researcher, who suggested the ‘amnesiac barrier’) - people that would usually reject a distortion will readily accept them in hypnosis, or they will be undetected
- People may remain in control, but may not be motivated to reject the suggestions, or not be motivated to take control back
- According to K. S. Bowers (another state-theory researcher)…
- Subjects enter a state of ‘uncritical receptivity’
- They experience a dissociation of control whereby suggestions directly activate responses automatically
- According to them, the subject may not only lose control, but may also be uncritical of it
- There’s the possibility that reals responded and didn’t realize the significance of their actions, while simulators responded for reasons of social pressure (etc)
- “Hoencamp (1992) argued that, through what he calls trance ratification, responsive hypnotic subjects may succeed in convincing themselves that they have lost control of their behavior, and this could result in a subjective experience of nonvolition and lead to their abuse.”
- From a non-state perspective, people can respond just to the pressure. People do weird things all the time with psychologists, doctors, military officers, game show presenters… etc. There’s a difference between compulsion / duress and automatism
- With hypnotic interviews - there were confessions, but they were generally later denied. In those sessions, there were also elements of coercion (deception, physical pressure, persistent questioning, and false friendship)
- Hypnotic procedures do not improve memory accuracy. In fact - they can increase confidence in false memories. Oops.
- Individuals in hypnosis are may susceptible to leading questions - producing information both correct and incorrect.
- Hypnotically created pseudomemories can be significantly reversed if there’s a suggestion that some ‘hidden part’ can describe their real memories. Pseudomemories clearly can and do occur, and these reversal techniques are not always effective.
- For reversal to occur, the demands (EG, telling someone else in the room vs an officer) must be sufficient to tell ‘the truth.’
- When given the suggestion to respond confidently and not be intimidated, subjects were less likely to reduce their level of confidence when interviewed.
- If you actually want to help someone remember something, use non-hypnotic techniques.
- It’s probably easier for someone to talk to a psychologist than a police officer. (A clinician, not a hypnotist.)
- Use a “cognitive interview…”
- context reinstatement (recalling thoughts and feelings)
- focused retrieval (try harder man)
- extensive retrieval (repeated retrieval efforts)
- witness-compatible questioning (tailoring the interview)
- (These also reduce the negative effects of standard police interviewing.)
- By itself, a guided memory procedure did not improve reacall, but hypnosis increased errors with no increases in accuracy.
12 - Self-Regulation Therapy - Suggestion Without Hypnosis
Section titled “12 - Self-Regulation Therapy - Suggestion Without Hypnosis”Salvador Amigo
- ‘Self-regulation therapy refers to a group of procedures that are based on the use of suggestion within a nonhypnotic context (i.e. in a “waking” state).
- Salvador Amigó PhD argues that suggestion without a hypnotic context is the essence of hypnosis, given the statistically effective CSTP takes a cognitive-behavioral approach to improving suggestibility.
- ESRT (emotional self regulation therapy) hinges on sensory recall, using a cognitive-behavioral styled approach to provide suggestions. This includes motivational instructions, instructions to think with suggestions, and procedures to teach people how to increase their responsiveness to suggestions. “For instance, participants were asked to extend an arm and observe the sensation of weight after the experimenter had placed an object in that hand. In later sessions they were asked to respond to arm-heaviness suggestions by recalling the sensations they had previously experienced.” ESRT has a different procedure than Sacks and Anderson’s approach, but the sensory-recall exercises have the same structure.
ESRT Overview
Section titled “ESRT Overview”- Phase 1: Give the reasoning behind the approach, then give a real physical stimulus, then ask them to recall and recreate them.
- Phase 2: Practice reproducing sensations without a physical stimulus aid.
- Phase 3: Practice generating new sensations without
Phase 1
Section titled “Phase 1”First, kick things off with the reasoning behind the approach. If you’re not collecting statistics, you’ll want to turn the following into a conversation. The wording’s pretty stiff.
The therapeutic procedure we will initiate is based on the mechanism of sensory recall. It is a mechanism that our brain uses regularly. For instance, it is possible that you recall certain memories, emotions, and even physical sensations from the past when you listen to a song that has a special meaning for you. Perhaps you heard that song many years ago when you declared your love to someone special or when a relationship ended. The song then became associated with that meaningful and deeply emotionally charged situation, so that when you listen to that melody today, its emotional and sensory components reappear immediately and automatically. With the help of the therapeutic procedure that I will teach you today, we will use the same sensory-recall mechanism for your own benefit.
Requires:
- A pail of ice water
- An ashtray with ‘fresh’ ashes
- A glass of lemon juice
- A heavy object (probably a book)
The four sensory exercises include…
-
Putting their hand in cold water
-
Holding a heavy book
-
Smelling cigarette ashes
-
Tasting lemon juice
-
Trial 1 - The clients are asked to just repeat an activity until they can clearly remember it.
-
Trial 2 - The clients repeat this, but are given a cue to think about and associate with the activity’s sensations.
-
Trial 3 - Use the cue to recreate the sensation.
Repeat the trials as much as needed to reproduce any of the sensations, then move on to another exercise.
Phase 2
Section titled “Phase 2”Reproduce some of the sensations from the exercises in the previous phase. However - this time, don’t use the previous ‘cue.’ For example, the journal entry provides…
As soon as you touch this pen, your hand will become rigid and numb.
Have the subjects practice this a few times, using associated images, thoughts, or internal cues. If you’re going by the book, don’t move on from phase 2 until direct suggestion is enough to create these sensations.
Phase 3
Section titled “Phase 3”Called the generalization phase…
Welp - according to the book, “any therapeutic suggestion should generate the suggested effects.”
ESRT - Short Version
Section titled “ESRT - Short Version”This is a shorter version. Instead of requiring some props, all you need is a heavy object.
You’ll be creating the following responses:
- Salivation
- Leg paralysis
- Arm heaviness
- Hand rigidity
Phase 1
Section titled “Phase 1”The wording here is uh. Awkward to say the least. If you want, you can look up the original article at Self-regulation therapy: Suggestion without hypnosis. (apa.org) - but trust me, you’re not missing much.
Hit the following points:
- Imagine you’ve got a piece of candy in your mouth and go to town licking away.
- Highlight that they’re salivating because of their physical movements, and this simulates tasting candy.
- Notice whatever sensations you notice in detail - remember them for later. Let them know that you’ll be asking them to reproduce those sensations.
- Give them as much time as they need to start salivating.
Once you have the go-ahead that they’re salivating, start with the next round of suggestions…
- Tell them to swallow in the least uncomfortable way possible. (Or screw it, I don’t know what your power dynamic is. Have fun!)
- Pre-frame that they just created this sensation through physical means, but they can do the same thing with sensory recall.
- Highlight that the following are very important…
- Don’t force anything by straining your concentration. Just think think and remember the sensations.
- Maintain an “open, relaxed, and trusting attitude without forcing the issue.”
- You’re not in a contest with anyone else. 😕
- You’ll see the benefits of this process soon.
- You’re taking advantage of your brain’s abilities - including those to associate and remember sensations.
- You’ll be able to remember at least some of the sensations on your first attempt.
- Actively reject interfering thoughts - such as “I can’t do this” or “this is silly.”
- Only concentrate on the sensations you’re about to experience.
- Ready? Sweet.
- Focus on those salivating sensations.
- Be calm, assured those sensations will appear.
- Don’t use any physical means to produce the sensation. (Or, you could say - “you don’t need to move or do anything physically to let these sensations return.”)
- Do whatever you’d like to help improve your concentration.
- You can close your eyes if you like, whatever helps.
- Get comfy.
- These steps don’t get in the way - in fact, they help!
- (Personally, I’d just say take as long as you need.)
- Wait for confirmation of the moist.

Sweet! They’ve achieved hypnotic phenomena!
- Praise them.
- Ask them what they noticed.
- Praise them again.
- Tell them to notice how the sensation keeps getting stronger and clearer, without any effort.
- Highlight that they did this by just thinking about it.
- Praise them. (Hopefully they have a praise kink.)
- They did perfectly, continue.
Leg Paralysis
Section titled “Leg Paralysis”Dr Amigó’s approach is a bit novel for inducing leg catalepsy!
- Have the subject plop their feet down flat on the ground, parallel to each other, with their hands resting on their knees.
- Ask them to press (gently) down on their knees with their hands, while trying to lift their their feet. (Note they should lift their soles, not just their toes.)
- When they notice they cannot lift their legs like this, ask them to notice the sensations of immobility so they can reproduce it later on.
- Give them a short break.
- Ask them to reproduce the sensations.
- Keep commenting on how well they’re doing.
Arm Heaviness
Section titled “Arm Heaviness”Following much the same structure.
- Have the subject extend their arm, and place a book in their hand.
- Ask them to notice any sensations (tension, discomfort, pressure, movement, the usual.) Instruct them not to fight the book taking their arm down.
- Ask them to reproduce it through memory or imagery.
- Reinforce as usual.
Hand Rigidity
Section titled “Hand Rigidity”- Have them lift their left hand, as if to make an oath.
- Have them push their fingers back with their right hand, leaving it in that mildly uncomfortable position.
- Ask them to notice how it feels (discomfort in the wrist, forearm, inability to move the hand, and general rigidity.)
- Give them a momentary break.
- Have them reproduce the sensations, the hand should go back to that bent position from the oath position without using the right hand.
- Praise them. “Because the results have been perfect,” it’s time to go to a more advanced stage.
Phase 2
Section titled “Phase 2”Just have the client reproduce the sensations without the physical precursor, since they’ve been memorized. Ask them to reproduce the sensations at will a bunch of times, shuffle it up, and highlight how these responses are automatic. Frame this as a kind of “mental workout” to improve these abilities. When they’ve mastered these, they can move on to a more advanced stage.
Phase 3
Section titled “Phase 3”Highlight that they’ve improved their ability to respond automatically, and because of this, they’ll be able to experience other sensations, even if they haven’t practiced them. Tell them this is because of the “mental workout” from earlier.
Give them the variety-pack of (easy) suggestions, as they can be experienced automatically. They mention…
- Hand warming
- Feelings of happiness and tenderness
- Nausea
- “Challenge” suggestions (inability to walk, move)
You can introduce therapeutic suggestions now. (But for god’s sake if you’re doing therapy or change-work, go read the original journal entry. It’s short.)
Give them a ‘signal’ for increased suggestibility for future sessions. For example - tell them that if they can make their hand rigid and cataleptic, they should be receptive to other suggestions as well. This is similar to rapid reinduction. You two can use whatever signal you want.
Application Considerations
Section titled “Application Considerations”- ESRT is never referred to as hypnosis, or any sort of special state of consciousness.
- Everything is just an exercise - if something “doesn’t work” this is treated as normal. You can repeat an exercise as many times as you need.
- The patient ‘must participate actively.’ This means they need to give feedback, propose ideas, propose solutions, etc.
- It’s crucial to praise and motivate your client.
- This is great for people that reject hypnosis.
Cases and Conclusion
Section titled “Cases and Conclusion”In the ending sections of this entry, there’s an exchange where the therapist directly suggests how gross the client finds cigarettes, acting and miming how disgusting it is. While the hold a single cigarette and hold it out to them to offer it to them, she swats the cigarette out of her hand, complaining that her stomach is turning. Entertainingly (and heartwarmingly,) the client talks about wanting to climb a mountain now that she’s quit smoking - and imagines herself doing so while climbing on the therapist’s table.
In another account, they spoke of a guy suffering from heroin withdrawal. I’m a bit skeptical of how genuine the subject was in this case, but he did say he was able to reproduce the positive effects of the high from heroin. He also suggested that his symptoms of withdrawal (headache, tremors, coldness) had disappeared completely. 🤔They had a follow up appointment in two weeks to check in, things seemed as if they were going fine. Three weeks after that, he went missing.
13 - Applications of Emotional Self-Regulation Therapy
Section titled “13 - Applications of Emotional Self-Regulation Therapy”Antonio Capafons
Holy crap boys - we made it to the end of the book.
I’m skipping over a lot of this - most of it is a repeat of what’s in Chapter 10. It might be useful to actual therapists and hypnotists doing changework.
- In Phase 3 of ESRT, this is where they show you can shift emotions. EG - Shifting from craving to disgust, then to indifference.
If ESRT fails initially:
-
Suggest the client interfered with it or they could not activate a sensory recall. (Hm, I’m not sure I’m down with this method. ) Tout the benefits of recall - they can use it to control a situation or stop something bothersome. (Or, if you’re in a recreational space, tell them that they did a good job in exercising their agency! And have them try again.)
-
Invite them to do a “learning exercise”
-
Wow dang. The book just instructs the therapist to hold the client down while they try to get up. (Or substitute a different sensory recall if this doesn’t work.) To be fair - they do reinforce that you should only do this if they’re all right with the process.
-
When they’ve verified that they can’t stand up, ask them to relive that on their own.
-
Tell them to…
- Eliminate that feeling and stand up.
- Talk about the feelings they had.
- Sit their ass back down and have them recreate that feeling.
- Suggest they say “stop” internally to stop the sensation.
-
Hypnosis is promising as part of a multimodal treatment (EG - don’t use JUST hypnosis.)
-
For the best outlook on hypnotic treatment, you’ll need… individualized suggestions, multiple sessions, a supportive therapist (probably you,) and high motivation from the individual
- Go figure, treatment efficacy seems correlated with high expectancies of it going well, skills for coping with stress, appropriate skills to deal with relapses, seeing yourself as an ex-smoker, and to be highly motivated
-
You need to take extra time during your first session to establish rapport and explain what you’re doing, as well as have them fill out questionnaires
-
The third and following sessions encourage them to adopt a nonsmoker role, stimulus control, self-monitoring, and setting up a quit day
Here’s some suggestion protips:
- Use a visual, tactile, or taste suggestion that cigarettes are nasty. Remind them of when they disliked the taste, felt dizzy, or whatever.
- Suggest they get the relaxing effects of smoking a cigarette from holding a pencil.
- Weirdly - use age regression to a time when they were nonsmokers.
- Ask them to smoke and hold it in. This is so they can ‘feel’ the aversion once or twice, not to do aversive conditioning
- You can also suggest that not smoking is “being like young again…”
- Suggest indifference. Change the urge into indifference, distance, and coldness.
- Do assertiveness training. Go offer them some crap cigarettes and let them smack it out of your hands. (If you’ve never hung out with smokers - get Pall Mall’s. They’re gross. You’d probably get the same reaction from someone not trying to quit.)
- Suggest the notice the improvements to their health, or be able to expect them.
- Suggest they are more easily satiated from smoking earlier. If they smoke actual cigarettes, have them mark ‘stop lines’ with a marker.
- Train relaxation.
- Suggest catalepsy when they try to grab a cigarette.
- “During the next 2 hours, I will not feel the urge to smoke” is better than trying to wish-away the addiction.
- Spiegel & Spiegel suggest focusing on the positives of not smoking rather than the negatives. (This makes sense - I’m having a tasty ass Oreo shake and if someone told me it’s going right to my thighs, I wouldn’t give a fuck. But, if they told me they’d give me a back massage to throw this thing out I’d do it in a heartbeat.)
- Find a trigger and have them roleplay it. “When you argue with me, really argue with [the name of the relative / that one flat earther]…” and remind them that they don’t need to smoke, they are upset, and they just need 15 minutes to relax.
- If you anchor a feeling of confidence or calm, make it subtle, like a thumb and the middle finger together. If they start chanting in the middle of a room they don’t need to smoke it’s gonna be pretty awkward.
- Research on this therapeutic package have been promising. (I don’t know if this means like - just the hypnotic and therapeutic sessions, or if it includes a helpingof prescribed Bupropion… ) The 6 month follow up had 66% success and 29% reduction. (The control group had 3% and 5%, respectively.)
Okay - so what about weight loss?
- ESRT is more appropriate for smaller amounts of weight. It might not help with morbid obesity.
- Really just… the same ideas from before.
Anything else?
- My gay-gray-ace-dumb-ass had to google what Dysmonorrhea was. But apparently it helps there.
- Someone was able to recreate the effects of MDMA with a cough drop, so that sounds pretty cool.
- This also works if you think flying sucks. They used suggestions of time distortion, time projection (?), indifference to flying in a plane (lol), boredom, and sleep. They used a video of flying on a plane to help make sure this works before doing the real thing and man that sounds terrible. XD Give me the cough drops.